ActiveVital: Geometry-Aware Embodied Vital Signs Monitoring for Home Healthcare Robots
A vision-guided mobile robot that orients its mmWave radar toward the chest, so respiration and heartbeat can be measured without contact. The key idea is to control the sensing geometry, not just process the signal.
The robot arm steers the radar toward the chest; as the alignment improves, the phase spectrum resolves into separate respiration and heartbeat peaks.
Application: non-contact respiration and heart-rate monitoring for home and companion robots, without wearables or user cooperation.
Abstract
Home robots require reliable vital signs monitoring to support long-term companionship and safety in daily environments, yet obtaining respiration and heart rate without physical contact remains challenging in unconstrained home settings. Millimeter-wave (mmWave) radar offers a promising solution due to its phase sensitivity to sub-millimeter motions. However, mmWave measurements are fundamentally constrained by observation geometry, since only the radial component of motion is observable. Consequently, arbitrary robot–human orientations often introduce angular misalignment that destabilizes vital signs estimation.
To address this limitation, we reformulate vital signs monitoring from passive signal recovery to active geometric regulation. We propose ActiveVital, a vision-guided sensing framework that treats sensing geometry as an explicit control variable for robots. It localizes the chest anchor via visual keypoints and converts alignment errors into control commands. This steers the robot-mounted radar toward near-normal incidence to the thoracic surface, maximizing radial observability within a perception–action loop. A differential phase enhancement module further stabilizes signal extraction under motion. Experiments show that ActiveVital reduces respiration interval error from 0.87 s to 0.14 s and heart rate error from 13.59 bpm to 2.22 bpm, achieving accuracy comparable to controlled static sensing while remaining robust under unconstrained robot–human configurations.
Key Insight: Sensing Geometry is a Controllable Variable
mmWave radar measures displacement only along its line of sight, so only the radial component of respiration and heartbeat motion is observable. Measurement quality is therefore governed by sensor–human relative pose rather than signal processing alone. Instead of asking the user to stay aligned, ActiveVital lets the robot actively regulate the observation geometry:
- (a) Static Sensing relies on user cooperation to maintain favorable geometry.
- (b) Proximity Embodied Sensing only reduces distance, leaving anatomical alignment unregulated.
- (c) Geometry-Aware Embodied Sensing (ours) actively controls sensor pose for chest-centric, near-normal alignment.
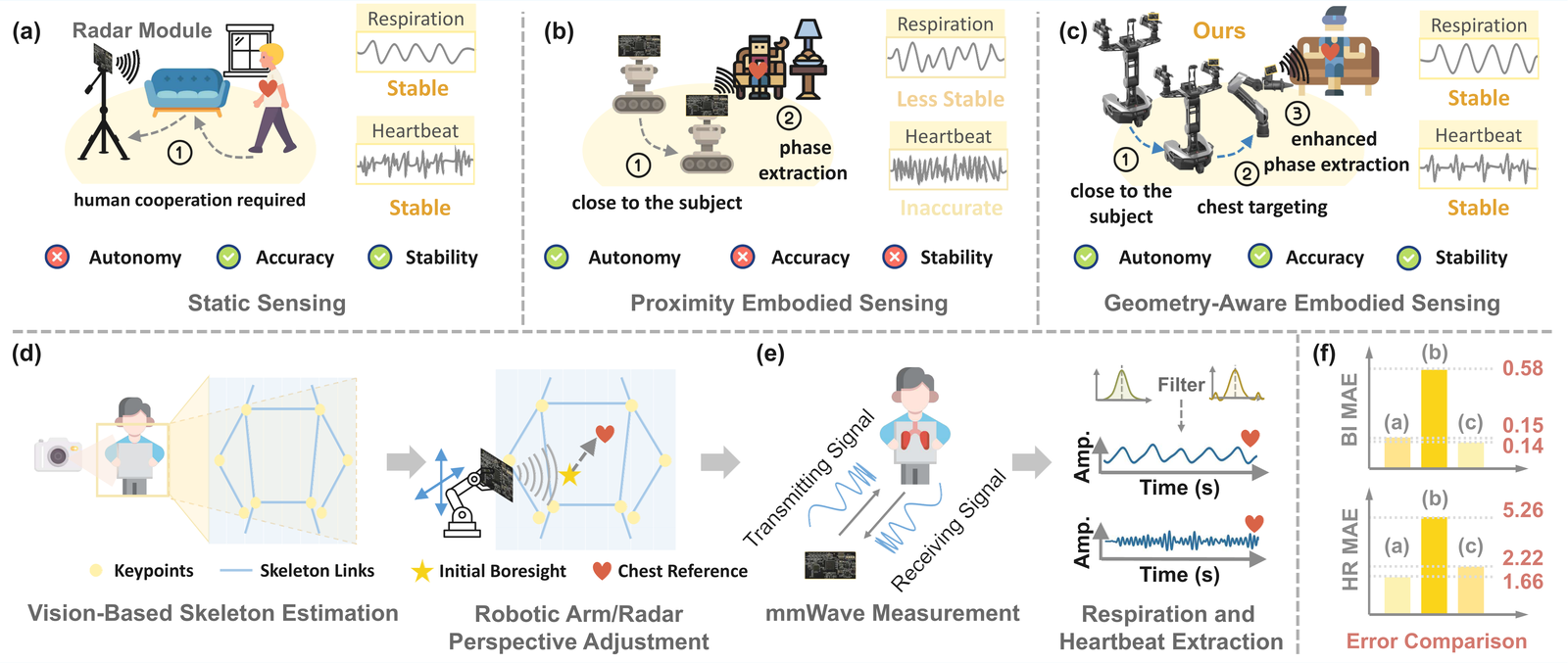
Vision-based chest localization and geometric reference estimation drive a closed-loop radar alignment that maximizes radial observability, yielding clearly separable respiration and heartbeat components.
Method
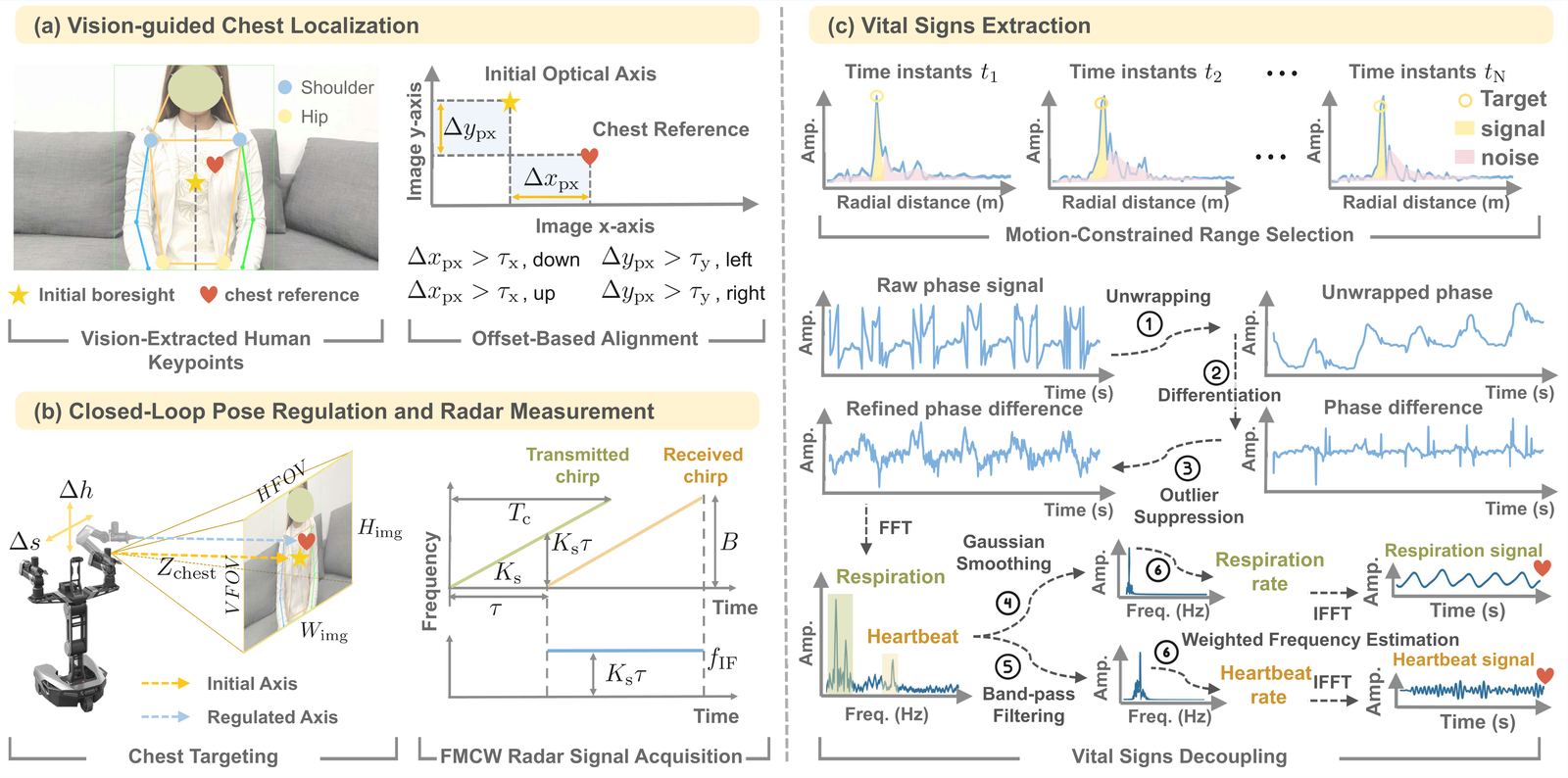
Processing pipeline: vision-guided chest localization → closed-loop pose regulation and FMCW radar acquisition → motion-constrained vital signs extraction.
ActiveVital resolves the geometry-induced observability constraint through a three-stage pipeline:
- Chest localization. ViTPose detects four torso keypoints (shoulders and hips) to define a chest-centered reference in the image domain, biased toward the upper chest and cardiac-adjacent region.
- Chest-centric observation construction. Pixel deviations between the radar optical axis and the chest reference become closed-loop motion commands, mapped to metric displacements via depth and camera intrinsics, steering the radar line-of-sight toward near-normal incidence (θ→0) to maximize radial observability.
- Geometry-constrained phase processing. Slow-time phase is unwrapped, differentiated, and cleaned with a Hampel filter (differential phase enhancement), then spectrally decoupled into respiration and heartbeat components for rate estimation.
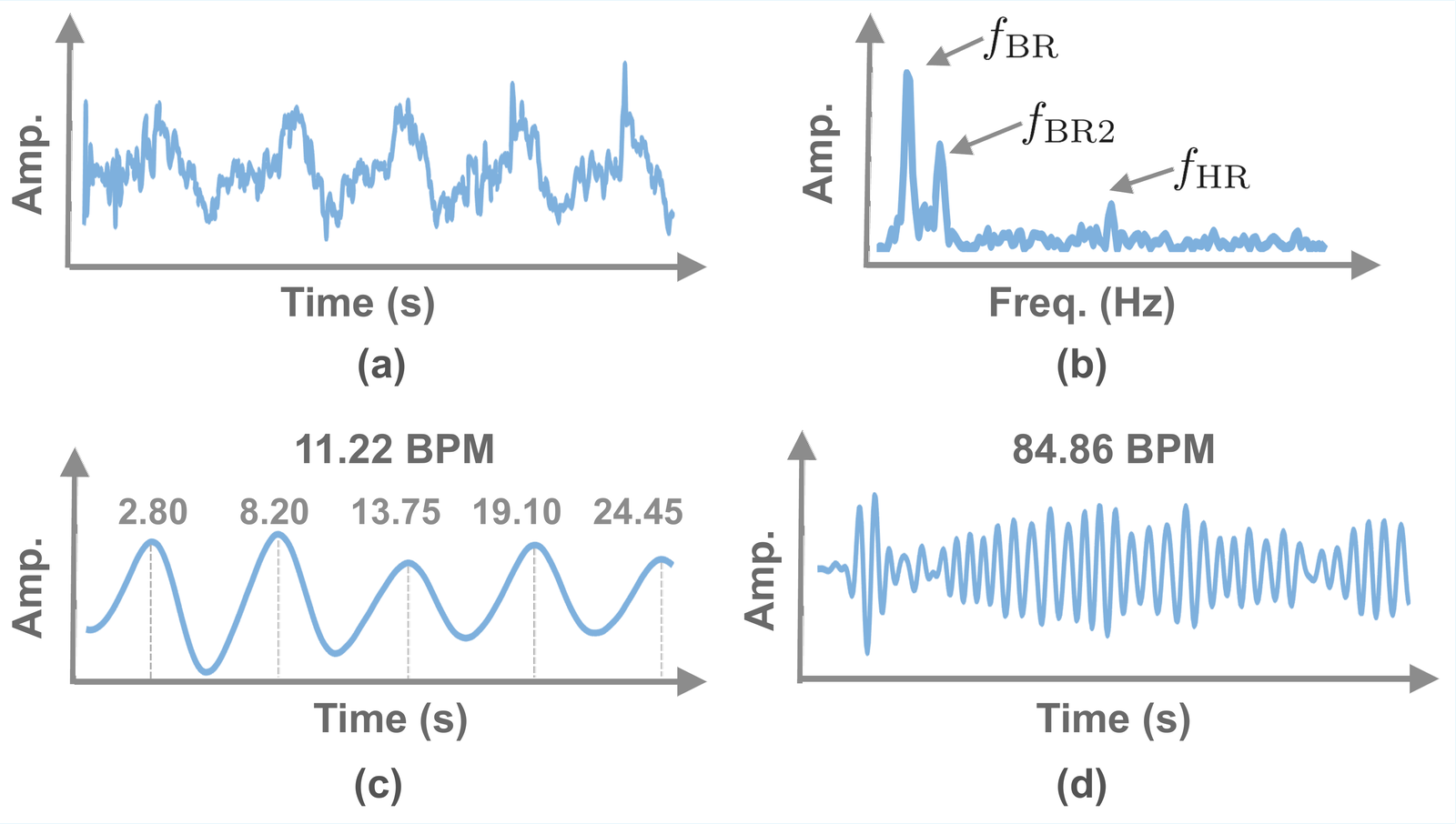
Observation Geometry Matters
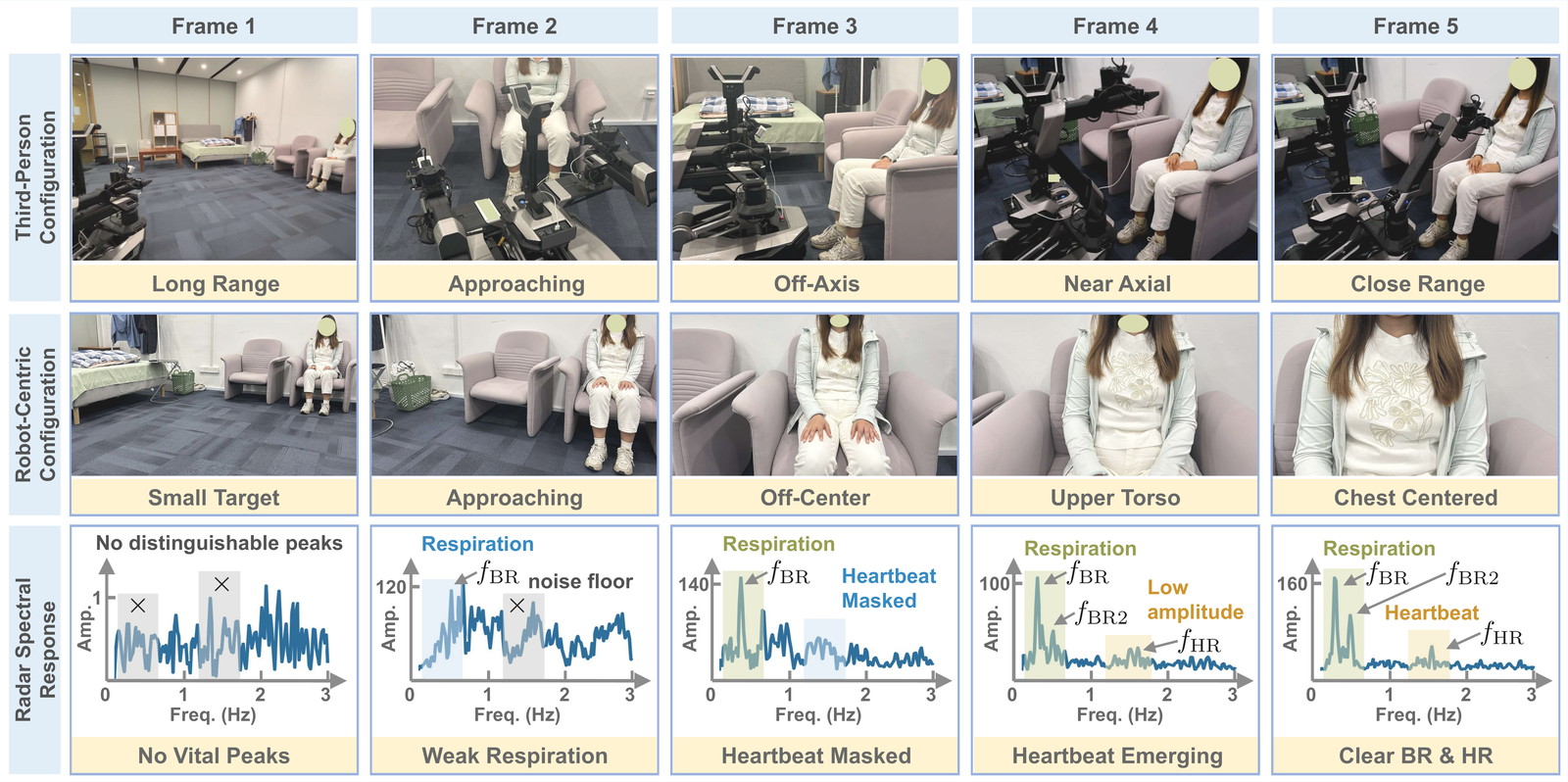
As the radar moves from long-range / off-axis conditions to chest-centered alignment, the phase-derived spectra transition from indistinguishable signals to clearly separable respiration and heartbeat components.
Proximity ≠ Alignment
Static & Proximity baselines
Static keeps peaks only with manual alignment; Proximity buries the heartbeat
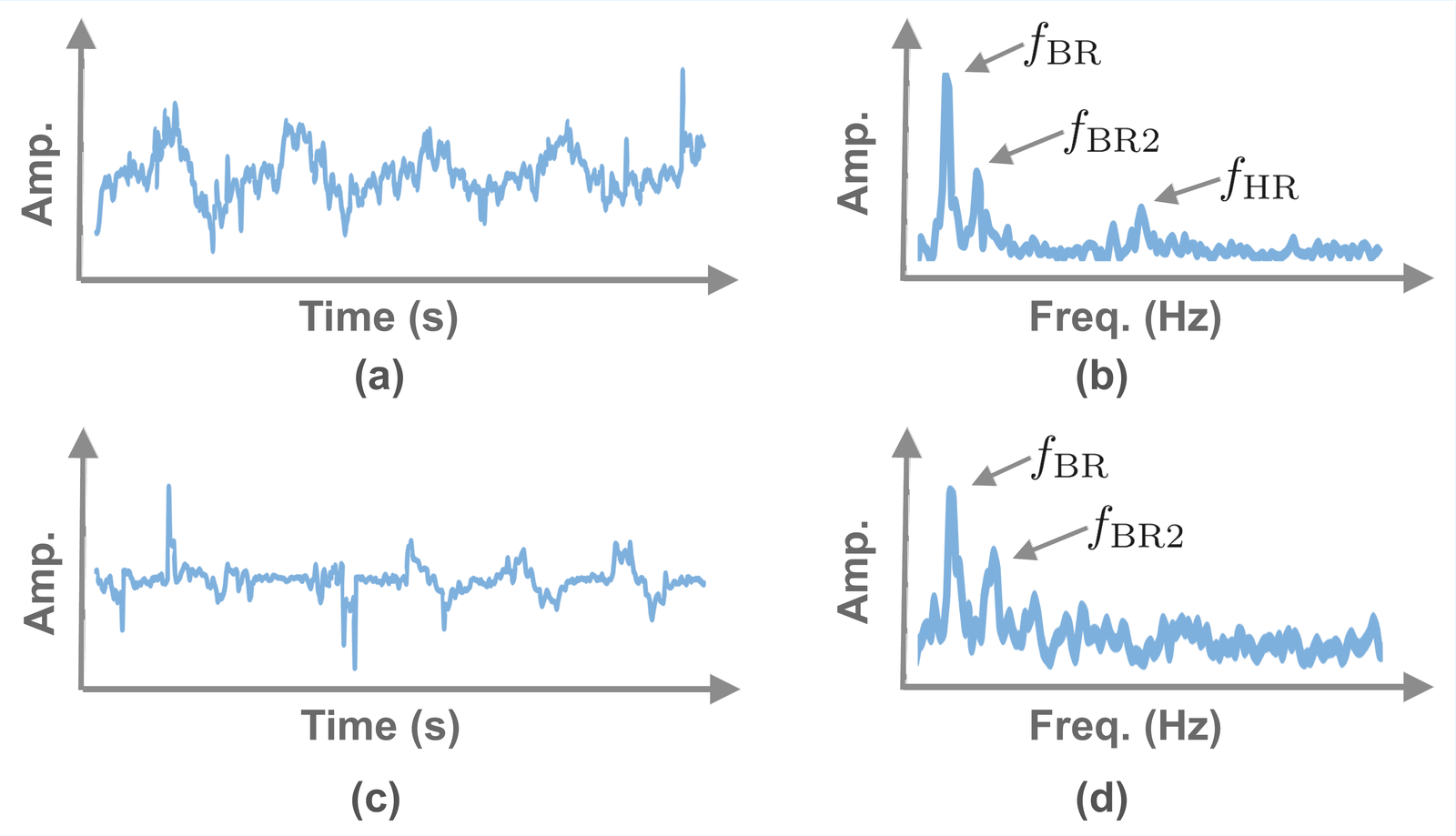
ActiveVital, geometry-aligned (Ours)
Respiration and heartbeat peaks clearly separated
Getting closer (Proximity) raises echo amplitude but does not fix the angle, so the heartbeat’s radial projection still collapses into noise. Only when the robot aligns the radar with the chest normal do the respiration and heartbeat peaks reappear. In this regime, observation geometry, not the signal-processing algorithm, is the limiting factor.
System & Hardware

ActiveVital is implemented on a Galaxea R1 Lite mobile robot integrating a 60 GHz FMCW radar (1T3R, 57.5–63.5 GHz, ~0.0228 m range resolution) rigidly mounted on the robot arm, together with an RGB-D camera for chest localization. A fingertip pulse oximeter provides heart-rate ground truth and an RGB camera provides respiration reference.
Results
Estimation across three sensing paradigms
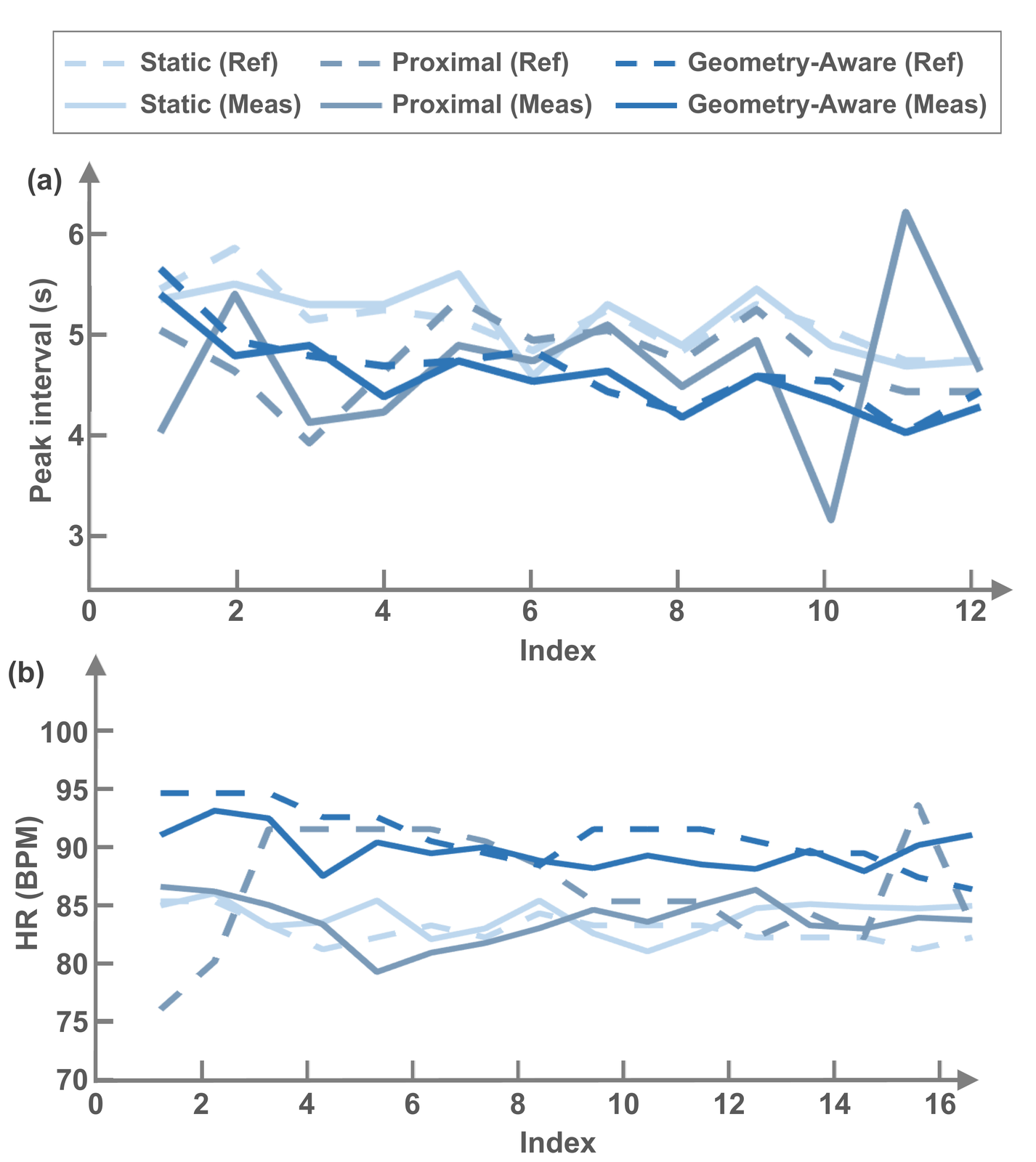
Breath interval (BI) and heart rate (HR) estimates vs. reference under Static, Proximity, and ActiveVital sensing.
Quantitative comparison across sensing paradigms
MAE / RMSE for BI and HR using our method
| Paradigm | BI MAE (s) | BI RMSE (s) | HR MAE (bpm) | HR RMSE (bpm) |
|---|---|---|---|---|
| Static | 0.15 | 0.19 | 1.66 | 1.96 |
| Proximity | 0.58 | 0.78 | 5.26 | 6.59 |
| ActiveVital (Ours) | 0.14 | 0.17 | 2.22 | 2.59 |
ActiveVital matches manually-aligned Static sensing without requiring subject cooperation, and clearly outperforms Proximity sensing.
Comparison across signal-processing algorithms
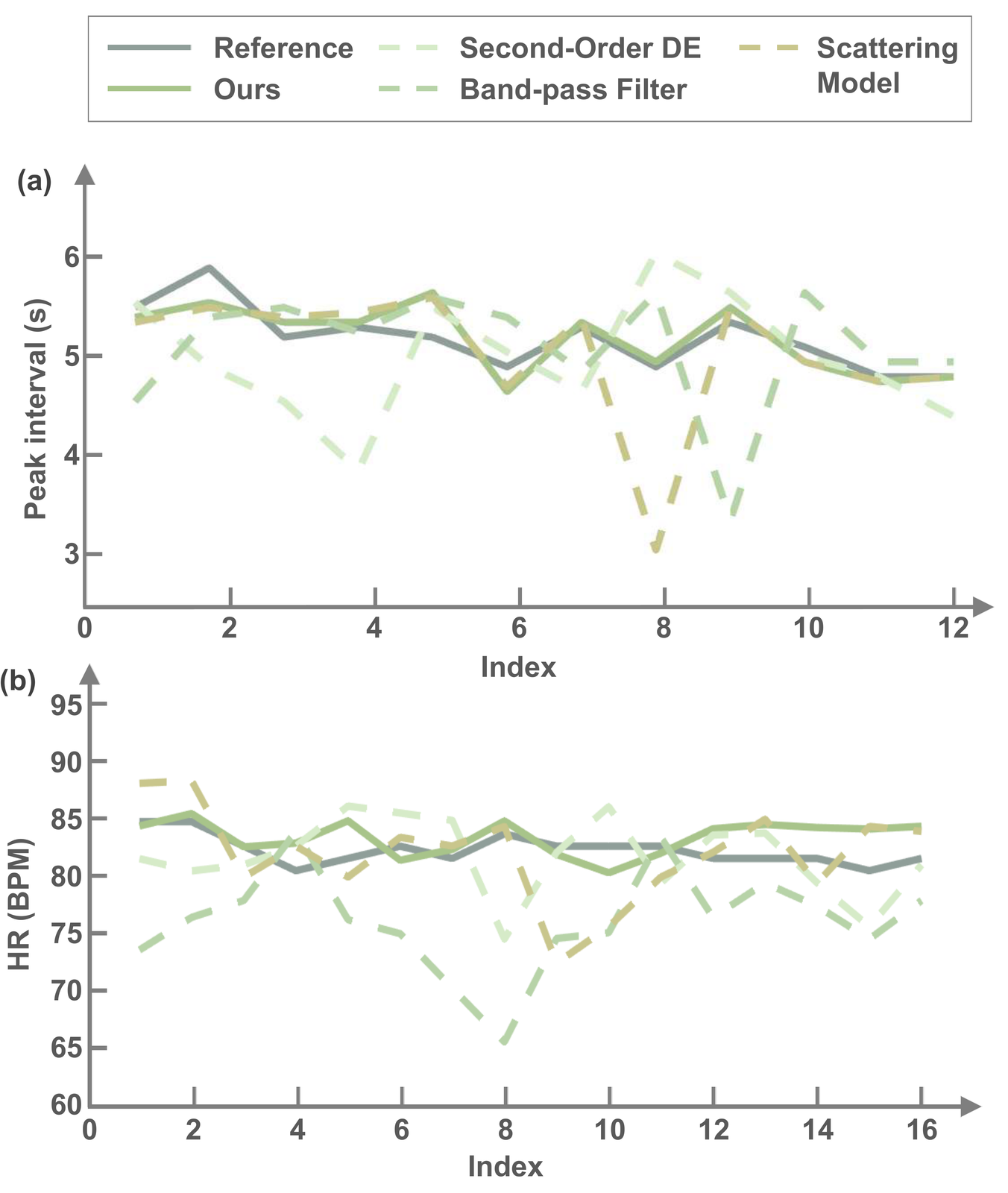
Under Static Sensing, our phase-refinement method is compared with three baselines for breath interval (a) and heart rate (b) against reference measurements.
Cross-algorithm comparison across the three sensing paradigms
MAE / RMSE — BI in seconds, HR in bpm
| Algorithm | Static | Proximity | Geometry-aware | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BI MAE | BI RMSE | HR MAE | HR RMSE | BI MAE | BI RMSE | HR MAE | HR RMSE | BI MAE | BI RMSE | HR MAE | HR RMSE | |
| Second-Order DE | 0.51 | 0.68 | 2.93 | 3.44 | 0.65 | 0.75 | 9.27 | 12.12 | 0.93 | 1.40 | 7.60 | 9.48 |
| Band-pass Filter | 0.56 | 0.75 | 6.29 | 7.36 | 0.87 | 1.18 | 13.59 | 15.07 | 0.30 | 0.37 | 14.48 | 15.88 |
| Scattering Model | 0.31 | 0.57 | 2.81 | 3.60 | 0.60 | 0.89 | 11.82 | 13.67 | 0.12 | 0.16 | 6.78 | 8.55 |
| ActiveVital (Ours) | 0.15 | 0.19 | 1.65 | 1.96 | 0.58 | 0.78 | 5.26 | 6.59 | 0.14 | 0.17 | 2.22 | 2.59 |
The proposed method degrades least as geometry deteriorates, preserving the weak cardiac-induced phase across paradigms.
Error distribution over 30 recordings
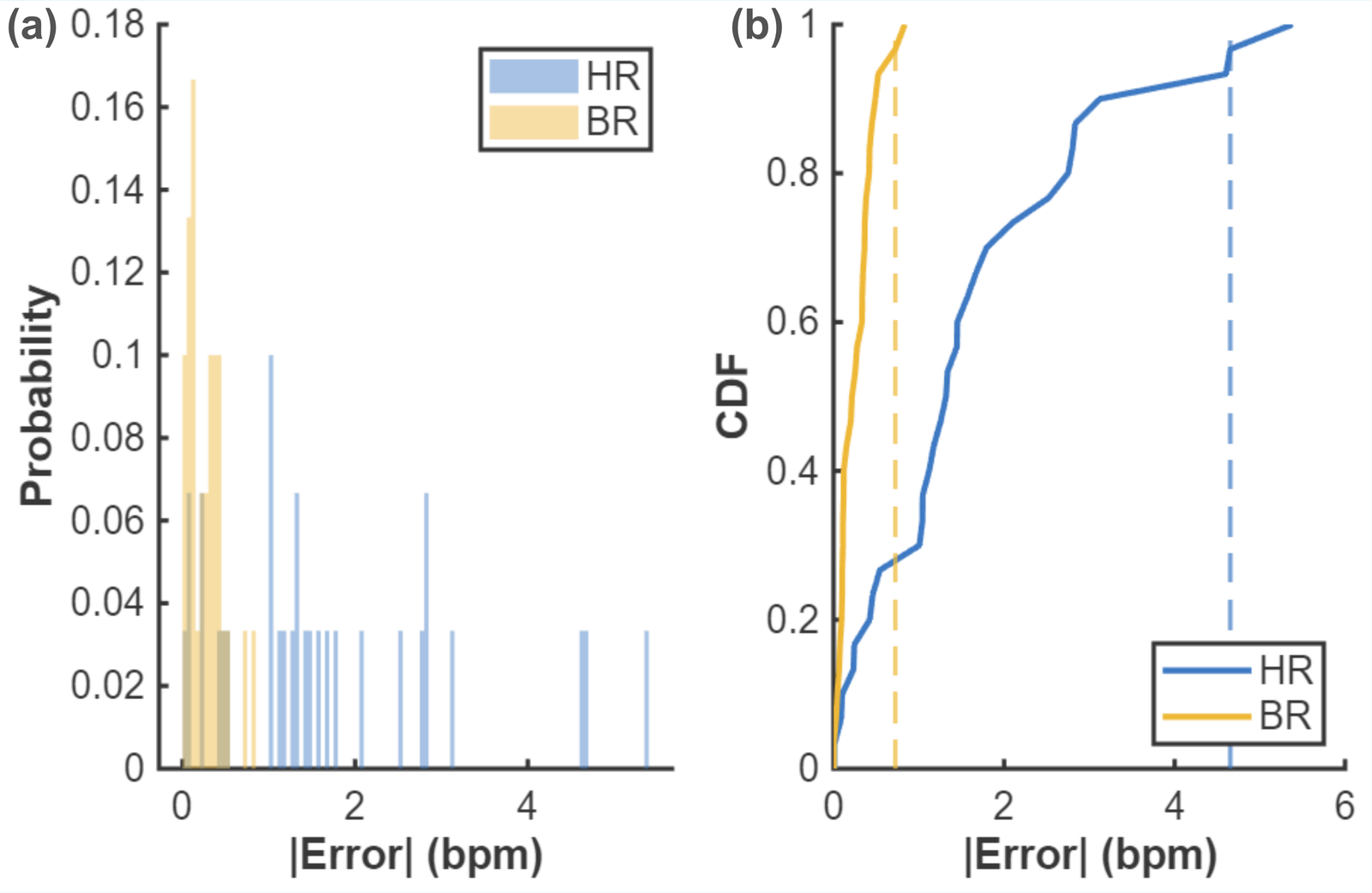
Histogram and CDF of absolute errors over 30 independent recordings (25 s each); dashed lines mark the 95th-percentile thresholds.
| Metric | MAE | RMSE | P95 |
|---|---|---|---|
| BR (bpm) | 0.26 | 0.33 | 0.72 |
| HR (bpm) | 1.67 | 2.16 | 4.65 |
BibTeX
@inproceedings{hu2026activevital,
title = {ActiveVital: Geometry-Aware Embodied Vital Signs Monitoring for Home Healthcare Robots},
author = {Hu, Yuxuan and Li, Shihao and Xiao, Yang and Li, Gen and Xu, Feng and Yang, Jianfei},
booktitle = {IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS)},
year = {2026}
}